A Longitudinal Analysis in Adolescence, Early Young Adulthood, and Young Adulthood
Trudy Festinger
James Jaccard
2012 New York University
Journal of the Society for Social Work and Research November 15, 2012
Volume 3, Issue 4, 280-295 ISSN 1948-822X DOI:10.5243/jsswr.2012.17
Data from 3 waves of the National Longitudinal Study of Adolescent Health, a nationally representative database, are used to test complex models addressing the developmental links between child adoption or non-adoption and suicidal ideation across adolescence, early young adulthood, and young adulthood. Diverse developmental dynamics are tested, while controlling for a variety of potential demographic confounds. Models are tested comparing kin and non-kin adopted youth to non-adopted youth, as well as the estimated effects of earlier versus later age at adoption to non-adoption. The models suggest modest differences in suicidal ideation during adolescence, early young adulthood, and young adulthood as a function of being adopted versus not-adopted and being adopted at age 4 years or later versus non-adoption.
During the past three decades, a substantial body of literature has accrued addressing outcomes among adopted children. Studies have focused on a number of outcome dimensions, for instance, children’s mental health (Wiersbicki, 1993); behavior, such as hyperactivity or oppositional behavior (Rushton & Dance, 2006; Sharma, McGue, & Benson, 1996; Simmel, Barth, & Brooks, 2007); educational achievement and social competence (Brodzinsky, Schechter, Braff, & Singer, 1984); and family structure, size, and sense of coherence (Barth & Brooks, 1997; Ji, Brooks, Barth, & Kim, 2010).
Results of all these studies comparing adopted youth (adoptees) to youth who were not adopted (nonadoptees) have been mixed, although analyses of nonclinical samples have tended to suggest that adopted children are at higher risk on a range of outcomes than their non-adopted peers (Brodzinsky, 1993; Miller, Park, & Winward, 2006). Such results do not necessarily implicate adoption itself, because the outcomes might be a function of other influences, such as (a) genetic risk for psychopathology, (b) prenatal risk, (c) postnatal-preplacement experiences, (d) characteristics of the adopted child or the adoptive parents, (e) the adoptive parent–child relationship, and (f) contextual variables (Miller et al., 2006). Regardless of cause, it is nevertheless important for professionals working in the adoption field to be aware of factors associated with having been adopted that might distinguish adopted children from their nonadopted peers, as these factors can inform intervention approaches and postadoption work with adoptive families.
In the mental health domain alone, a number of studies have addressed such areas as externalizing disorders (Bramlett, Radel, & Blumberg, 2007; Ingersoll, 1997; Keyes, Sharma, Elkins, Iacono, & McGue, 2008; Nalavany, Ryan, & Hinterlong, 2009; Simmel, Brooks, Barth, & Hinshaw, 2001), attachment security and relationship difficulties (Feeney, Passmore, & Peterson, 2007), and identity formation concerns (Grotevant, 1997; Wilson, 2004).
Overall, the history of these studies has suggested that “adopted children are at greater risk for adjustment difficulties compared to their non-adopted community-based peers” (Palacios & Brodzinsky, 2010, p. 273), although such comparisons show more similarities than differences (Haugaard, 1998), indicating the effects were not very strong.
Studies have also generally shown that adoptees more often manifest externalizing symptoms such as attention deficit hyperactivity disorder or oppositional and conduct problems rather than internalizing disorders, such as depression or anxiety (Palacios & Brodzinsky, 2010). Few large-scale studies with longitudinal designs have focused on internalizing dimensions. All of these gaps led us to the following general research questions: Is suicidal ideation more prevalent among adoptees than non-adoptees? Do ideation differences change over time as a function of adoption versus non-adoption status?
Literature on Depression and Suicidal Ideation Among Adoptees
Most recently, large general population datasets have examined the adjustment of adoptees. For instance, according to the 2007 National Survey of Adoptive Parents (Vandivere, Malm, & Radel, 2009), which compared 763 foster care, 781 domestic, and 545 international adoptees, “9 percent of all adopted children ages 2 and older have ever been diagnosed with depression compared to 4 percent of children in the general population” (p. 25). The percentages are higher in older children. Thus, 18% of adopted children ages 12 to 17 have ever been diagnosed with depression compared with 7% of children in the general population. No particular differences in proportions of children with depression were noted between foster care, domestic, and international adoptees.
Longitudinal approaches to adjustment also have been reported. Early studies, for instance by Bohman and Sigvardsson (1990), used Swedish registers of children beginning around the time of their births and followed early adoptees and schoolmate-comparison children into young adulthood. Results showed “increased frequency of nervous disturbances and maladjustment” (Bohman & Sigvardsson, p. 104) during childhood and early adolescence, but showed few if any differences by late adolescence and young adulthood when compared with non-adoptees.
Many studies have reported on adoption and level of depression (i.e., Borders, Penny, & Portnoy, 2000; Brodzinsky, Schechter, Braff, & Singer, 1984; Keyes et al., 2008), and have frequently found a somewhat higher rate of depression among adoptees. However, the main thrust of the analysis presented in this article is on suicidal ideation. In what follows, we summarize studies with a focus on suicidal ideation rather than a primary focus on depressive symptoms.
An early New Zealand study (Fergusson, Lynskey, & Horwood, 1995) concerned adoptees that were part of a 16-year longitudinal study, the Christchurch Health and Development Study, that followed a birth cohort of 1,265 children born in mid- 1977. A variety of measures were administered to 14- to 16- year-olds, including 32 adoptees, 842 youths in two-parent families, and 60 youths in single-parent families. The investigators reported no significant differences in the rates of suicidal ideation or behavior among these adoptees and non-adoptees after adjusting for a variety of family social background factors and perinatal history.
A Swedish study (von Borczyskowski, Hjern, Lindblad, & Vinnerljung, 2006) used the National Swedish Register to follow a cohort of 7,340 domestic and 6,065 international adoptees for 15 years (1987 to 2002). These researchers noted that, after adjusting for gender, age, and socioeconomic status, both adoptee groups showed an increased risk of suicide attempts and suicide deaths when compared with non-adoptees.
Similar findings were reported by a Danish study (Petersen, Sorensen, Mortensen, & Andersen, 2010).
This study used the Danish Adoption Register to compare cause-specific mortality for a number of causes, including suicide, among 14,425 non-kin adoptions completed over a 23-year period beginning in 1924. The study reported an excess mortality rate with respect to suicide among adoptees when compared with the general Danish population.
It is, of course, unclear whether the results observed for youth in Sweden, New Zealand, and Denmark generalize to U.S. youth. In the United States, several investigators have examined adoptees’ risk for attempted suicide using data from the National Longitudinal Study of Adolescent Health (Add Health; Bearman, Jones, & Udry, 1997; Harris, Halpern, Whitsel, Hussey, Tabor, Entzel & Udry, 2009). For instance, Slap, Goodman, and Huang (2001) used Wave 1 Add Health data (when most respondents were between 12- and 17-years old) to focus on a subset of adolescents who had never been separated from their mothers for more than six months, were living with their adoptive or biological mothers, and “the adoptive mother had never been married to the adolescent’s biological father” (p. 1). Slap et al. compared their sample of 214 adoptees with the 6,363 non-adoptees and, after adjusting for depression and aggression, reported the adoptees were more likely to have attempted suicide; a result not mediated by impulsivity. Feigelman (2001) also used Wave 1 Add Health data but reached a different conclusion. He compared 369 adolescent adoptees in two-parent families with 9,676 non-adoptees in twoparent families, and with 7,457 children in step- or single-parent families. Feigelman noted, “suicide ideation and attempts did not vary greatly among the three subsets of male and female adolescents” (p. 18).
A few years later, Feigelman (2005) used multiple waves of Add Health and focused on a comparison of 346 non-kin adoptees with approximately 14,000 nonadoptees. In this later study that examined suicidal ideation, suicide attempts, and depression levels, Feigelman found essentially no compelling significant differences between non-kin adoptees and nonadoptees.
Present Study
Because Add Health used a large, nationally representative sample, the data set is useful for exploring mental health differences between adopted and non-adopted children. The adoption questions asked in Wave 1 of the Add Health survey (administered when adolescents were in Grades 7 to 12) were plagued by psychometric problems regarding the accurate self-identification of who was an adoptee (Fan et al., 2002; Feigelman, 2005).
However, most of these deficiencies were remedied when respondents were interviewed about six years later during early young adulthood. The present study capitalizes on Add Health’s longitudinal design that interviewed youth during adolescence (Grades 7 to 12, when most youth were between 12- and 17-years old), again during early young adulthood (approximately six years after the first interview), and again during young adulthood (approximately 12 years after the first interview). The longitudinal focus of the present study on three distinct developmental periods is unique relative to past adoption research. The research extends the prior work of Feigelman by using covariates as well as longitudinal modeling that better represents the multivariate dynamics at play.
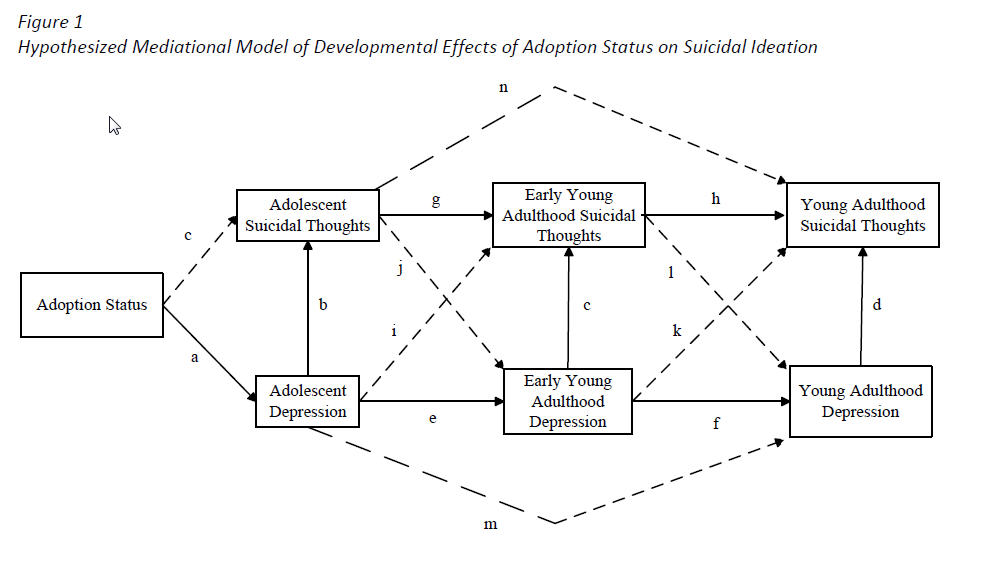
The working model that guides the analysis is shown in Figure 1. Whether an individual was adopted was assumed to impact suicidal ideation during adolescence by virtue of its effect on adolescent depression (path a), which, in turn, affects suicidal ideation (path b). The link between depression and suicidal ideation (path b) has been well established in past research (e.g., Kandel, Raveis, & Davies, 1991; Mazza & Reynolds, 1998). Accordingly, it is reasonable to conceptualize depression as a theoretical mediator of the presumed effects of adoption status on suicidal ideation. However, it is unclear whether adoption status affects suicidal ideation independent of depression; therefore, we placed a dashed arrow for path c in Figure 1, indicating that a theorist could make a case for either the presence or absence of that causal dynamic in the model. Prior research has not explored this issue. Consistent with the inclusion of path b in the model, a contemporaneous path linking depression to suicidal ideation also is posited at each of the other developmental stages (see Figure 1, paths c and d). Figure 1 also includes first-order autoregressive effects across time for both depression (paths e and f) and suicidal ideation (paths g and h). Autoregressive effects exist when a variable at a prior point in time exerts a direct effect on that same variable at a later point in time. A first-order effect occurs when this causal dynamic involves consecutive time periods, such as the effect of depression at time (t) on depression at time (t + 1). The autoregressive effect for suicidal thoughts in Figure 1 implies that suicidal thoughts during adolescence predispose an individual towards suicidal thoughts during early young adulthood, which, in turn, predispose the individual for suicidal thoughts in later young adulthood. A similar dynamic is implied for depression; that is, prior experiences of elevated depressive symptomology predispose an individual toward such depressive expressions at later points in time characterized by the developmental periods under investigation. Although studies of the longitudinal structure of suicidal ideation have linked prior suicidal thoughts to future suicidal thoughts (e.g., Batterham & Christensen, 2012; Fordwood, 2007), thereby making these paths theoretically plausible, none of this research has spanned the particular developmental periods used in the present study. This limitation is also true for studies of depression (e.g., Essau, Lewinsohn, Seeley, & Sasagawa, 2010; Peirce, Frone,Russell, Cooper, & Mudar, 2000).
Figure 1: Hypothesized Mediational Model of Developmental Effects of Adoption Status on Suicidal Ideation
Ignoring the dashed paths in the model for the moment (we discuss these paths below), we now elaborate substantive implications of the hypothesized contemporaneous and autoregressive effects.
Model Implications
Developmental dynamics. The hypothesized contemporaneous and autoregressive effects imply interesting developmental dynamics. To illustrate, the model in Figure 1 predicts that adolescent depression should be associated with suicidal ideation some six years later, during early young adulthood. This association occurs because of two mediational chains.
First, adolescent depression contemporaneously increases the tendency for an adolescent to engage in suicidal ideation (path b), and, in turn, this suicidal ideation during adolescence increases the tendency to engage in suicidal ideation six years later during early young adulthood (path g). The causal chain pb–pg (where this notation is read as “path b through path g”) thus links adolescent depression to suicidal ideation six years later. In fact, the model also predicts that adolescent depression will continue to be associated with suicidal ideation some 12 years later during young adulthood by virtue of the hypothesized (autoregressive) effect linking suicidal ideation in early young adulthood to suicidal ideation in young adulthood (see the mediational chain pb–pg–ph).
The second dynamic contributing to the link between adolescent depression and suicidal ideation six years later is adolescent depression affecting later depressive tendencies during early young adulthood (path e), which, in turn, have a contemporaneous effect on suicidal ideation (path c). This effect reflects the mediational dynamic of pe–pc.
In sum, according to the model in Figure 1, adolescent depression is presumed to be associated with suicidal ideation six years later by virtue of the chain pb–pg and the chain pe–pc. The association of adolescent depression with suicidal ideation extends out some 12 years into young adulthood by virtue of the chain pe–pc–ph as well as pb–pg–ph . and, indeed, also through the chain pe–pf–pd. To the extent that adoption versus non-adoption is associated with depression during adolescence, then this association will cascade throughout the model via the various causal paths and manifest itself in differences in suicidal ideation during early young adulthood and young adulthood. We would expect these effects to become diluted as an individual progresses through increasingly distal meditational dynamics; nevertheless, the model has potentially nontrivial developmental implications. The present research tests whether the Add Health data are consistent with a model that contains these developmental dynamics and estimates the magnitude of the presumed effects by virtue of examination of relevant path coefficients.
Lagged effects. Lagged effects (paths i through l) are theoretically plausible and these are shown in Figure 1 with dashed arrows. These paths allow for reciprocal causal dynamics between depression and suicidal ideation over time. For example, depression during adolescence might predispose youth towards suicidal thoughts during young adulthood independent of the contemporaneous and autoregressive effects already discussed (path i). Similarly, suicidal thoughts during adolescence might predispose youth to depression during early young adulthood independent of the other influences in the model (path j). With respect to the former dynamic, little research has explored the lagged effects implied by Figure 1 for depression on later suicidal ideation, especially across the developmental time periods we focus on. To be sure, prior research has shown that depression predicts future suicidal ideation (e.g., Kandel et al., 1991; Mazza & Reynolds, 1998), but whether this effect is mediated by future depression or operates independent of future depression has not been well documented.
For example, Shahar, Bareket, Rudd, and Joiner (2006) did not find evidence for such effects, but they focused on a small convenience sample from a clinical population and obtained measures over a total span of only six months. By contrast, our focus is on a national sample across three significant developmental periods—adolescence, early young adulthood, and young adulthood. Depression during adolescence might start an individual down a trajectory of poor academic performance, and hence, lowered future educational attainment as well as weakened interpersonal ties with significant others, all of which can translate into future feelings of isolation. These delayed manifestations might impact future suicidal ideation tendencies independent of expressions of concurrent depressive symptoms. Whatever the mechanism, a useful first step is to document whether data are consistent with the presence of such lagged effects, and our modeling efforts explore this possibility. If lagged effects are present, then future research and theorizing can address the unique mechanisms that account for such effects. In addition, such paths would represent additional mediational chains by which adopted versus non-adopted youth would be predicted to differ in future suicidal ideation.
Second order autoregressive effects. The final theoretically plausible causal dynamic is the presence of second-order autoregressive effects, as reflected by paths m and n in Figure 1. Consider path m, which links depression during adolescence to depression during young adulthood, independent of depression during early young adulthood. The hypothesis is that the experience of depression during adolescence has an impact on the adolescent’s life in ways that take time to manifest as depressive symptoms in young adulthood relative to early young adulthood. For example, perhaps patterns of cognition learned during adolescence persist and affect ways of perceiving and interpreting intra- and interpersonal events into young adulthood, independent of changes in life circumstances during early young adulthood (e.g., moving away from home, increased freedom and sense of responsibility). The presence of such second-order effects represents another mediation chain through which adoption status might have an impact on suicidal ideation during early young adulthood and young adulthood. We also tested whether a model with such effects is consistent with the data.
In sum, the present research evaluates complex models of the developmental links between adoption status and suicidal ideation across adolescence, early young adulthood, and young adulthood. The research extends prior research by embedding adoption status and suicidal ideation into a multivariate, longitudinally dynamic class of models with contemporaneous effects, autoregressive effects, and lagged effects, with a nationally representative sample of youth. The research chooses between models that posit different developmental dynamics and describes the implications of those models that are most plausible vis-à-vis the Add Health dataset, which uses a nationally representative sample. Given the multivariate, longitudinal character of this research that grounds statistical analyses, the research extends prior work that has tended to rely on more simple bivariate associations.
More Fine Grained Analyses of Adoption Status
One reason results across previous studies may have been disparate is because of the way adoption status has been conceptualized and measured. Some research has compared children who were adopted versus those who were not, with no further distinctions. Research has shown that being adopted by kin differs qualitatively from being adopted by non-kin (e.g., Howard & Smith, 2003; Ryan, Hinterlong, Hegar, & Johnson, 2010), that being adopted at a young age differs qualitatively from being adopted later in childhood (e.g., Festinger, 2005; Hjern, Lindblad, & Vinnerljung, 2002; Smith & Howard, 1999), and that being adopted internationally differs qualitatively from being adopted domestically (e.g., Groza & Ryan, 2002; Juffer & IJzendoorn, 2005; Keyes et al., 2008). The present research makes such distinctions when comparing adopted with nonadopted youth in the context of the Figure 1 model.
Another problem with some adoption research is that it has tended to ignore demographic confounds that might affect the observed differences in suicidal ideation between adopted and non-adopted children. These variables include education, family income, age of the child, ethnicity, and parental marital status. The present research controls for these confounds during the modeling enterprise.
In sum, the present research extends prior work by (a) comparing adopted versus non-adopted youth on suicidal ideation using a large, nationally representative sample of adopted youth who were studied across three important developmental periods (adolescence, early young adulthood, young adulthood); (b) evaluating models of the longitudinal dynamics surrounding suicidal ideation in adopted versus nonadopted youth that include contemporaneous, lagged, and autoregressive effects that respect the complex mediational dynamics through which such youth might differ in suicidal ideation over time; (c) introducing controls for a host of demographic covariates that might have biased parameter estimates in prior research that failed to control for them; (d) examining the role of depression as a mediator of adopted versus not-adopted differences in suicidal ideation, including whether these differences persist independent of depression; and (e) making distinctions between different forms of adoption (e.g., kin vs. nonkin, age of adoption) when comparing adopted and non-adopted youth on suicidal ideation. In addition, the research should yield interesting perspectives on numerous (as yet to be explored) longitudinal dynamics between depression and suicidal ideation across three core developmental periods independent of whatever insights it yields on adoption differences in suicidal ideation.
Method
Respondents
The study used data from Add Health (Bearman et al., 1997; Harris et al., 2009), a large scale, nationally representative data base that initially interviewed 20,745 adolescents in Grades 7 to 12. The sampling frame used a random sample of 80 high schools stratified by region, urbanicity (urban, suburban, rural), school type (public, private, parochial), ethnic mix, and size. For each high school, a set of feeder schools, which included seventh graders, was identified. Some high schools included Grades 7 to 12 and functioned as their own feeder school. In all, 134 discrete schools were studied.
Approximately 200 adolescents were selected from each of the schools, including several strategic oversamples (e.g., Black students whose parents had a college degree). Sampling weights were derived by Add Health statisticians to permit inferences for a nationally representative sample. We used a set of specialized longitudinal weights for the three waves subject to analysis in this study. A parent, in most cases the resident mother, was asked to complete a questionnaire covering topics that overlapped with the adolescent questionnaire and included information about the economic status of the household.
The sample was reinterviewed approximately six years later and then a third time about six years after that. The general age range of students was 12 to 17 years at Wave 1 (adolescence), 18 to 23 years at Wave 2 (early young adulthood), and 24 to 29 years at Wave 3 (young adulthood). Of the original sample, 71% (n = 14,738) were interviewed at Wave 2, and 73% (n = 15,197) were interviewed at Wave 3. There were no notable biases in attrition. Sampling weights for Waves 2 and 3 adjusted for attrition to maintain national representativeness of the sample across waves (Chantala, 2006).
Detailed questions about adoption status were asked of youth at Wave 2, when they were about 18- to 23-years old. The screening questions used to identify adoptees asked respondents whether they were adopted, and if so, whether the adoption was by a step-parent due to remarriage. The latter group of adoptees was not included in our analyses. We identified 532 adoptees for purposes of analysis. Relying on self-reports for adoption status means we do not include adopted individuals who were unaware of, or did not admit, their adoptive status by early young adulthood; however, such individuals are probably relatively few in number. In the analyses reported below, sample sizes deviate somewhat from the 532 adoptees because some cases did not have sampling weights, some cases were missing data, and because of skip patterns.
Procedure
At Wave 1, Add Health in-home interviews were conducted with students and the responding parent (usually mothers). Data were recorded on laptop computers. The Add Health interviewer read the questions and entered the respondents’ answers. Questions on sensitive topics were administered using audio computer-assisted self-interviewing methods that allowed respondents to use earphones to listen to prerecorded questions and enter their responses directly into the computer. Respondents were assured of the confidentiality of their responses and were told they could skip any questions they felt uncomfortable about answering. The interview included a wide range of topics, such as health status, health facility use, nutrition, peer networks, decision-making processes, family composition and dynamics, educational aspirations and expectations. Adolescents were interviewed for each data wave. Parents were interviewed for Wave 1 only. The same general interviewing strategy was used at all waves.
Measures
Depressive symptoms. Expression of depression symptomology was measured at each of the three waves using the Center for Epidemiologic Studies Depression Scale (CES-D: Radloff, 1977), which is a widely accepted instrument used for assessing depressive symptoms in adolescent and adult populations (Brooks & Kutcher, 2001; Field, Diego, & Sanders, 2001; Franko et al., 2005; Richards & Perri, 2002; Wilcox, Field, Prodromidis, & Scafidi, 1998).
The long version of the CES-D is a 20-item scale that asks respondents to indicate the frequency with which they have experienced certain feelings or situations. For each situation or emotion, the item asks the respondent to consider “how often you have felt this way during the past week” and responses are rated on a 4-point scale ranging from rarely or none of the time (less than 1 day), which is coded 0, to most or all of the time (5–7 days), which is coded 3. Higher scores indicated greater severity of depressive symptoms.
Add Health used a shorter 10-item version of the scale that is highly correlated (r = .85) with the full scale (Jaccard, 2003). The alpha coefficients for the measure in our analysis were 0.80, 0.81, and 0.82 at Wave 1, Wave 2, and Wave 3, respectively. Averaging items makes the CES-D scores scale more interpretable. For example, a score of 2.1 means that the average response for an individual was near the response option occasionally or a moderate amount of time (3–4 days) across the 20 items. Past research that summed rather than averaged responses to the CES-D suggests that CES-D total scores over 16 are consequential and near formal depression (Radloff, 1991). A score of 16 maps roughly onto a score of 0.80 on our metric that used averaged rather than summed responses.
Suicidal thoughts. Suicidal ideation was measured at all three waves by a single item: “During the past 12 months, did you ever seriously think about committing suicide?” Response options were yes (coded 1) and no (coded 0).
Adoption status. The Wave 2 survey included a series of questions about adoption, including (a) “Were you ever adopted?” Positive responses triggered follow-up questions of (b) “Were you adopted by a blood relative?” (c) “Were you adopted by a new spouse of one of your biological parents?” (d) “How old were you when you were adopted?” and (e) “Was this an international adoption—that is, were both of your adoptive parents living in the United States and you were living in another country?” Adoption questions also were asked at Wave 1, but these questions have been found to be suspect (Miller et al., 2001), so we did not rely on them.
Covariates. The covariates in the model analyses included three variables from the youth data—youth’s age, ethnicity, gender—and three variables from the parent data—mother’s educational attainment, parental marital status, and household income.
Analytic Strategy The data were analyzed using structural equationmodeling (SEM) as applied to panel data using theMplus 6.1 computer program. For weighted analyses,the complex sample option within Mplus was used toapply the sampling weights provided by Add Healthstatisticians (Chantala, 2006). In addition, statisticaladjustments were made for clustering because schools(rather than individuals) were the primary samplingunits (see Chantala, 2006). Model fit was evaluatedusing both global fit indices (the comparative fit index[CFI], the standardized root mean residual [SRMR],the root mean square error of approximation[RMSEA], and its associated p value for close fit[PCLOSE]) and focused fit indices (modificationindices, standardized residuals between predicted andobserved covariances). A robust estimator based onthe Huber-White sandwich estimator was used toaccount for nonnormality and is fundamental to thestatistical algorithm for clustered designs in Mplus.
For the dichotomous variable of suicidal thought, data were modeled using a modified linear probability framework, which has advantages in SEM relative to more traditional logit and probit analyses (Cheung, 2007; Daniloski, Jaccard, & Brinberg, 2011; Williams, 2009). Statisticians have questioned logistic regression for consequential assumptions of variance homogeneity and the standardized nature of logistic coefficients (Alvarez & Brehm, 1995, 2002; Williams, 2009; Yatchew & Griliches, 1985). We therefore used the modified linear probability model with a Huber- White robust estimator as implemented in Mplus. Simulation studies have suggested this approach is reasonable in a wide range of analytic scenarios (Cheung, 2007; Jaccard & Levitz, 2012). Missing data were handled using full information maximum likelihood methods (Enders, 2010). Loss of respondents to attrition was about 30% across the three waves of data collection. The sampling weights adjusted for any evident bias due to attrition.
Results
Preliminary and Descriptive Analyses
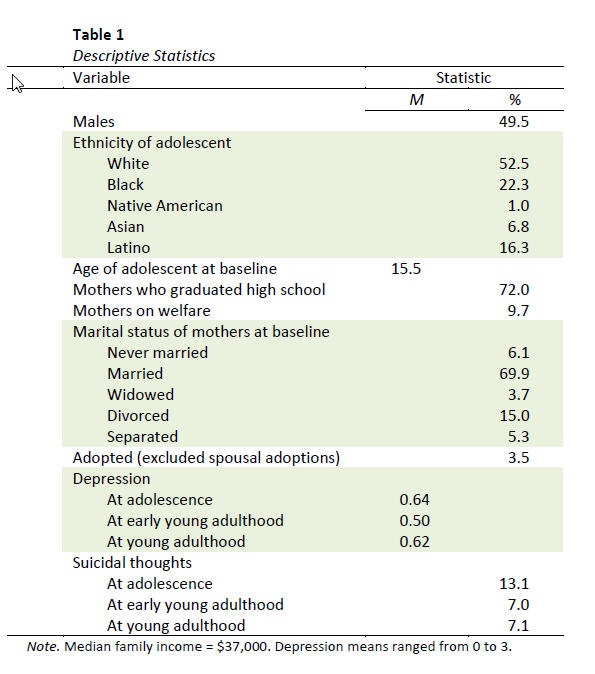
Table 1 presents (unweighted) demographic information for the full Add Health sample as well as (weighted) means for the core variables in Figure 1. Only 13 youth reported being adopted internationally. Given the small sample size, no further analyses were pursued comparing international with domestic adoptions. We eliminated all adopted youth who were spousal adoptions (e.g., youth adopted by the new spouse of the biological mother). Two remaining adoption categories were of primary interest: (a) youth adopted by kin (e.g., aunt, grandmother, uncles) versus youth adopted by non-kin, and (b) youth adopted at a relatively young age (i.e., younger than 4 years) versus youth adopted at an older age (i.e., 4 years or older). Although sample sizes were somewhat larger for cross-sectional analyses within a given wave, the working sample sizes for the longitudinal analyses were 311 kin adoptions, 111 non-kin adoptions, 325 adoptions at younger than 4 years, and 92 adoptions after or at age 4 years.
For the age-based categories, treating age as a dichotomous variable is suboptimal. We did so because we did not have confidence in the precision of youth self-reports about the age they were adopted. For example, we did not fully trust the age difference between youth who reported being adopted at 2 years old versus youth who reported being adopted at 3 years old, because it seemed unlikely that the youth would have remembered this information with such precision. We conducted extensive analyses on the age of adoption variable to determine appropriate cut-off values for defining meaningful groups. For example, our analyses revealed few differences on depression among youth adopted at 0, 1, 2, or 3 years of age, but we observed an upward shift in depression starting with youth adopted at 4 years and older, but few differences among the groups of youth adopted at 4, 5, 6 years and so on. Therefore, we worked with a dichotomous implementation of this variable, with a cut off adoption age of 4 years.
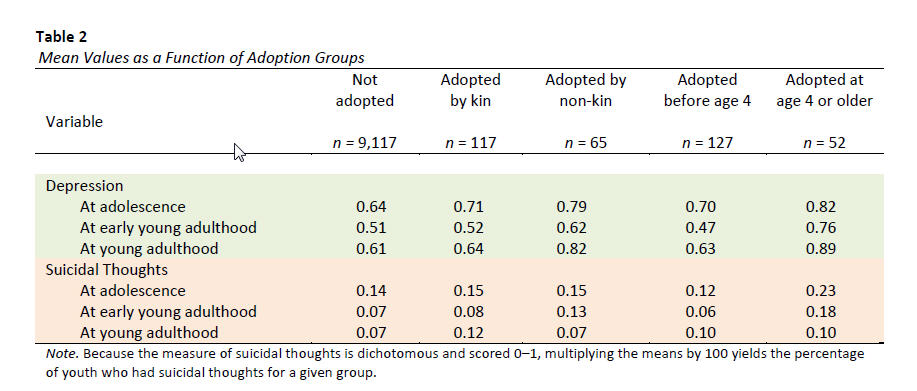
Table 2 reports the weighted mean values of the core variables in Figure 1, calculated cross-sectionally at each wave using the full sample information available at that wave as a function of the various adoption groups. Because the variable suicidal thoughts is dichotomous, the mean reflects the proportion of youth who had suicidal thoughts If multiplied by 100, it reflects the percentage of youth with suicidal thoughts. Means on the outcomes differ somewhat from the longitudinal analyses reported later because Table 2 calculations are cross-sectional in character within waves and do not include covariates. We do not report significance tests for the data in Table 2 because contrasts in the longitudinal analysis have more statistical power, take into account covariates, and exploit the multivariate information in the data. We therefore defer consideration of relevant tests and parameter estimates until later. It was not feasible to form all possible combinations of the two adoption categories (non-kin adoptees who were adopted before 4 years of age; non-kin adoptees who were adopted when 4 years of age or older; kin adoptees who were adopted before 4 years of age; kin adoptees who were 4 years of age or older at adoption) and have adequate sample size for trustworthy parameter estimates.
Therefore, we chose to conduct two separate SEM analyses; one in which adoption status was operationalized as kin/non-kin adoptions versus not-adopted, and a second analysis in which adoption status was operationalized as earlier/later age of adoption versus not-adopted.
Structural Equation Models
Kin/non-kin adoption versus non-adopted status. The model in Figure 1 with only solid arrows was fit to the data. All disturbances or residuals were assumed to be uncorrelated. The adoption status variable was defined by two dummy variables. The first dummy variable was kin adoption (scored as 1) and everyone else (scored 0), and the second dummy was non-kin adoption (scored 1) and everyone else (scored 0). Thus, youth who were not-adopted constituted the reference group. All the covariates described earlier were included in the model for each endogenous variable. The model is statistically over identified, and yielded a somewhat mixed performance on indices of overall model fit (χ2 = 228.49, df = 18, p < .05; RMSEA < 0.04, PCLOSE > .05; CFI = 0.94; SRMR= 0.018). Probes of sources of ill fit in the model examined modification indices (which document the extent to which the fit of the model is improved by adding a specified path; see Kline, 2010) and the standardized differences between the predicted and observed covariances (which indicate pairs of variables where the model fails to reproduce well the correlation between them; see Kline, 2010). These diagnostics suggested the revised model in Figure 2, which includes some of the dashed paths from Figure 1. The revised model yielded a good model fit for the global fit indices (χ2 = 24.63, df=14, p < .05; RMSEA < 0.009, PCLOSE > .05; CFI = 1.00; SMRM = 0.006). Probes based on more focused indices of fit (modification indices and standardized differences between the predicted and observed covariance) also yielded results consistent with good model fit. Figure 2 presents the unstandardized path coefficients for the model. In the model, kin/non-kin adoption status was assumed to have a direct effect on adolescent depression. The estimated effect was statistically significant for kinversus not-adopted youth (mean difference (MD) = 0.12, z = 2.09, p < .05) but not quite for non-kin adopted versus not-adopted youth (MD = 0.12, z = 1.87, p < .07). The estimated mean differences for the two contrasts were identical (both were 0.12), with the differential significance patterns being an artifact of the group sample sizes. When both groups were pooled to maximize power (which seemed justified given identical mean values in the two groups), the single degree of freedom contrast between the pooled kin and non-kin groups and the non-adopted youth was statistically significant (MD = 0.12, z = 2.81, p < .05). This estimated effect then reverberated to all other variables in the model through the various mediational chains of statistically significant path coefficients via the logic of joint significance tests as outlined in MacKinnon, Lockwood, Hoffman, Est, and Sheets (2002). For example, the pooled kin/non-kin versus not-adopted mean depression difference translates into differences in adolescent suicidal thoughts through the chain pa–pb (Figure 1). As another example, the pooled kin/non-kin adopted versus not-adopted mean depression difference translates into differences in young adulthood suicidal thoughts through the chain pa–pb–pg–ph (Figure 1) as well as a host of other chains that terminate with suicidal thoughts at Wave 3 and as reflected by all statistically significant path coefficients in those respective chains. Several of the implied causal chains in Figure 2 have interesting developmental implications, but we defer their consideration to the Discussion section.
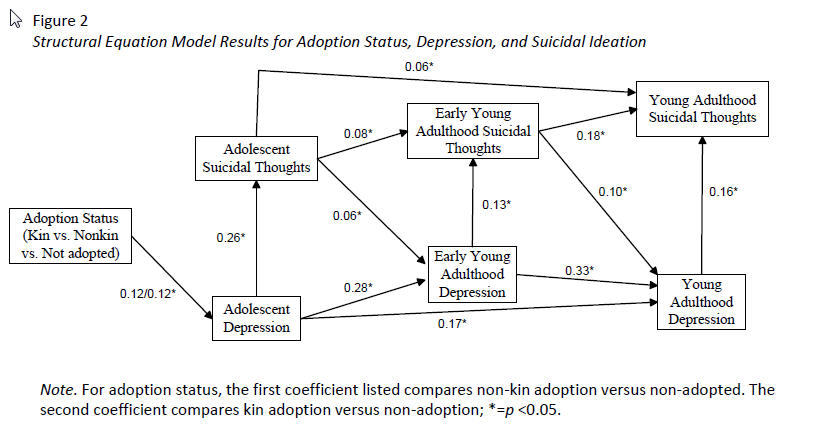
Although there were statistically reliable differences between adopted (pooled kin/non-kin) and youth who were not-adopted on the variables in Figure 2, the estimated effects on suicidal thoughts were small for the most part. For example, the estimated total effect for comparing pooled kin/non-kin adoptions to non-adopted youth on suicidal thoughts during young adulthood was only 0.01, indicating that 1% more kin/non-kin adopted youth than non-adopted youth had suicidal thoughts. The total effect for suicidal thoughts during early young adulthood was only 0.007 (or < 1%). The total effect for suicidal thoughts during adolescence was somewhat larger 0.032 (or 3.1%), indicating that 3.1% more kin/nonkin adopted youth than non-adopted youth had suicidal thoughts.1
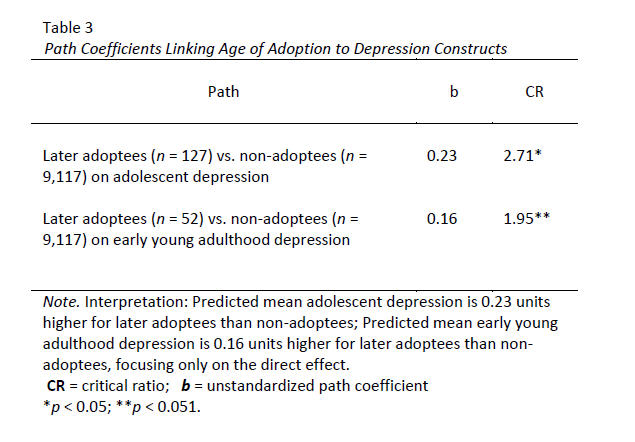
Early age of adoption versus later age ofadoption. The model in Figure 2 was reanalyzed, replacing the dummy variables for kin adoption and non-kin adoption with dummy variables for early adoption (1 = adopted earlier than age 4, 0 = everyone else) and later adoption (1 = adopted at age 4 or after, 0 = everyone else). As in the earlier model, the reference group was youth who were not-adopted. The model in Figure 2 with kin/non-kin adopted versus non-adopted youth overlaps considerably with this model. In fact, all the paths are redundant between the two models except for the single path linking adoption status to adolescent depression (because adoption status is now operationalized as non-adopted versus early/later adoption instead of non-adopted versus kin/non-kin adopted). The fit of the model was good (χ2 = 21.69, df = 14, p < .09; RMSEA < 0.01, PCLOSE > .05; CFI = 1.00; SRMR = 0.006), but more focused fit statistics (modification indices and standardized differences between the predicted and observed covariances) suggested one modification relative to the kin/non-kin versus non-adoption model, namely, the addition of a causal path from the adoption status dummy variables directly to depression during early young adulthood independent of the adolescent variables. With this path added to the model, the parameters were then re-estimated. The global fit indices of this model were good (χ2 = 18.46, df = 12, p < .10; RMSEA < 0.01, PCLOSE > .05; CFI = 1.00; SRMR = 0.005). Because there was so much redundancy between the results in Figure 2 and the current model, we focused attention on the path coefficients that are unique to the present model (otherwise, consult the path coefficients in Figure 2). The relevant information for these unique coefficients is presented in Table 3. None of the path coefficients for the dummy variables comparing early adoption to nonadopted youth were statistically significant. The path coefficient comparing adolescent depression for later adoptions to non-adopted youth was statistically significant (path coefficient, which reflects a mean difference, = 0.23, z = 2.71, p < .05). The (added) path coefficient comparing early young adult depression for later adoptions to non-adopted youth was nearly statistically significant (path coefficient = 0.16, z = 1.95, p < .051). This latter coefficient suggested that youth adopted at later ages tended to have higher levels of early young adulthood depression than nonadopted youth. Given the other statistically significant chains in the model, both of these effects reverberate through the other (statistically significant) paths to ultimately have an impact on suicidal thoughts during early young adulthood as well as young adulthood.
As with the prior analysis, although statistically reliable, the estimated effects of adoption status on suicidal thoughts were small in magnitude. For later adoption versus non-adoption, the estimated difference in suicidal thoughts was 2.9% higher during young adulthood for later adopted youth, 3.4% higher during early young adulthood and 3.5% higher during adolescence.2
Discussion
The present study yielded numerous interesting findings, some of which pertain to adoption dynamics and others that concern developmental dynamics more generally, independent of adoption.
Adoption Dynamics
The current research used an SEM-based longitudinal modeling approach to analyze associations between adoption status and suicidal ideation. This approach incorporated information about a core mediator, depression, into the modeling, thereby taking into account a fuller array of information than simple bivariate modeling of adoption status and suicidal thoughts. The models included autoregressive and lagged effects, making the analyses more thorough and multivariately grounded as compared with past studies of adoption that have used longitudinal data.
The results of our analyses were consistent with a model that posits differences in suicidal ideation during three developmental periods—adolescence, early young adulthood, young adulthood—as a function of adoption status. However, the modeling suggested that the somewhat heightened risk of suicidal ideation might depend on the characteristics of adoptees, namely, children who are adopted at age 4 years or later relative to non-adoptees. Prior research has tended not to make this distinction, has failed to include covariates, has used bivariate as opposed to multivariate modeling, and has relied on convenience samples. Thus, the results of the present research help to place the earlier work into a clearer perspective.
Although we observed several statistically reliable differences in suicidal ideation, the estimated effects were modest in magnitude, typically hovering around a 1% to 3% increased rate of suicidal ideation. Such differences might not be large enough to meaningfully affect either clinical practice or policy. Certainly, other indicators of suicide risk are more potent prognosticators of suicidal tendencies than adoption status. Having said that, researchers and practitioners probably should remain cognizant of the small increased risk of suicidal ideation for certain types of adoptees. In 2010 alone, more than 50,000 children were adopted from public foster care, which does not include the many international, independent, and private adoptions (Vandivere et al., 2009). A 1% to 3% increased rate of suicidal ideation, accumulated across all later adopted youth over a period of years, translates into thousands of individuals with suicidal inclinations. The many adoptive parents whose adopted children experience such thoughts almost certainly would not want this serious matter dismissed as a “small” effect size. Adoption advocacy groups might also take cognizance of these results in efforts to increase support for post-adoption services. The estimated longitudinal differences between kin/non-kin adoptions or later adoptions as compared with non-adopted youth were made in the context of a model with complex mediational chains involving autoregressive effects for depression, autoregressive effects for suicidal ideation, and lagged effects of prior suicidal ideation on later depression. Many of the developmental dynamics at work implied by the models operate independent of adoption status, so we consider them in the next section. The fact that suicidal inclinations were only modestly heightened as a function of adoption status renders somewhat moot the consideration of complex mediational chains that might produce those differences. Such interpretation is further mitigated by the fact that selection mechanisms might have operated, which makes it difficult to attribute differences in suicidal tendencies to adoption in the first place. Stated another way, assignment to the various adoption groups is not random, creating difficulties for causal inference. For example, children who are adopted later (age 4 years or thereafter) might experience late adoptions because they are more prone to having developmental disabilities (e.g., Glisson, Bailey, & Post, 2000; McMurty & Lie, 1992; Schmidt-Tieszen & McDonald, 1998) and these disabilities might be driving the observed (small) differences in suicidal tendencies rather than factors associated with the adoption experience.
Broader Developmental Dynamics
Independent of the observed adoption associations, several general developmental trends in the data are noteworthy. One intriguing result (see Table 1) is the pattern of means for depression and suicidal thoughts across the three developmental periods. For depression, mean depression scores were elevated during adolescence (M = 0.64) and then decreased during early young adulthood (M = 0.50).
This decline in depression from adolescence to early young adulthood has been observed in numerous studies (e.g., Pettit, Lewinsohn, Seeley, Roberts, & Yaroslavsky, 2010). However, what has not been previously documented is the subsequent upswing in depression during young adulthood (M = 0.62). The bases of this upswing are unknown and warrant future investigation.
Although we observed an upswing in depression, this was not the case for rates of suicidal thoughts, which dropped from adolescence (13%) to early young adulthood (7%) and remained at that rate during young adulthood (7%). Perhaps the increased maturity of young adults dampens the translation of depression to suicidal thoughts; that is, because of young adults’ increased maturity, the heightened levels of depression during young adulthood are not translated as readily into suicidal thoughts as compared with depression during adolescence. This should be explored in future research.
For both depression and suicidal thoughts, we found evidence for a second-order autoregressive model, which suggests experiencing depression and suicidal thoughts in adolescence may start youth down a trajectory toward increased risk in young adulthood that is independent of the increased risk due to the first-order autoregressive effects. The bases of these effects require the attention of future research. It may be, for example, that depression and suicidal thoughts during adolescence affect friendship patterns that later translate into reduced levels of social support, whereas adolescent-established friendships maintain long-term for young adults who were not depressed adolescents.
Finally, our data were consistent with a model in which suicidal thoughts at a prior developmental stage predispose youth to depression at a later developmental stage (see the lagged paths in Figure 2). For example, having suicidal thoughts during adolescence predisposes an individual towards increased depression during early young adulthood independent of prior levels of depression during adolescence.
Similarly, having suicidal thoughts during early young adulthood predisposes an individual towards increased depression during young adulthood independent of prior levels of depression during early young adulthood. In the minds of youth, suicidal ideation is likely noteworthy and memorable. The negative affect associated with these memories might be more readily accessible at later points in time (e.g., during early young adulthood), which, in turn, exacerbates the salience of cognitions relevant to depression. As with the other results in this section, the bases of these effects need to be explored in future research.
Limitations
As with any research endeavor, methodological and analytic limitations must be kept in mind when forming conclusions. Results can differ depending on statistical algorithms used to make inferences, methods for treating missing data, and the choice of variables to include as covariates, suggesting care is necessary when drawing conclusions, especially for effects that are marginally statistically significant. The measures of adoption status were based on self-reports by the adoptees and these reports might be subject to error, particularly for the reports of age of adoption.
The use of multivariate modeling is both a strength and a possible source of concern. To the extent that the models are correctly specified, then inferences of associations through the logic of joint significance tests are more efficient (in a strict statistical sense) than simple bivariate modeling. However, if there is specification error, then bias can result. For longitudinal models, issues of correlated versus uncorrelated disturbance terms are always of concern. The tested models assumed uncorrelated disturbances.
When we introduced correlated disturbances into the system, none of the correlations were statistically significant, which is an argument for excluding them. In the final analysis, possible specification error should always lead the analyst to interpret complex SEM models with caution.
The model estimates based on the multivariate data were at times slightly at odds with the descriptive differences reported in Table 2. This likely occurred for several reasons. First, the estimates at a given Wave in Table 2 were based on sampling weights for cross-sectional analyses within that Wave. By contrast, the longitudinal model parameter estimates used longitudinal weights deemed appropriate for multivariate longitudinal modeling. Second, the results were based on different sample sizes, due to attrition and missing data. Third, the multivariate model used covariates in the analysis, whereas the simple descriptive statistics in Table 2 did not.
Although Add Health is a large, nationally representative study, once we began defining meaningful adoption subgroups based on the complexities of adoption dynamics, sample sizes quickly dwindled to the point at which statistical power was compromised and parameter estimates became unstable. The subgroups we analyzed were judged to be of reasonable enough size to permit meaningful analysis, at least when comparing the adopted youth subgroups with non-adopted youth. Future research would benefit from stratified sampling designs that oversample theoretically important adoption groups for purposes of comparative analyses within the adopted groups and with non-adopted youth. The present research should be interpreted as support for such subgroup analyses, but not definitive with respect to subgroup differences.
Directions for Future Research
Despite the limitations, the present research yielded insights into associations between adoption status (adopted vs. non-adopted) and suicidal thoughts. The research also provided new perspectives on developmental phenomena relevant to suicidal ideation and depression that merit further exploration.
Future research should investigate and elaborate on the following:
- Whether and how different types of adoption experiences (beyond those explored in the present research) might raise or lower suicidal thoughts relative to non-adoptees (such as what we found with age of adoption),
- The mechanisms that account for the modeled cascading effects through the various longitudinal causal paths characterizing both depression and suicidal ideation across time, including
- the intriguing second-order auto-regressive effects for both depression and suicidal thoughts (whereby experienced suicidal thoughts and depression during adolescence predispose young adults to experience such tendencies, independent of their experiences in early young adult-hood; and
- the estimated lagged effect of suicide ideation on depression some six years later, independent of past depression.
- Identifying why depression decreases, on average, from adolescence to early young adulthood but then rebounds to higher levels during young adulthood, a pattern of mean shifts that does not mirror shifts in suicide ideation.
- Such questions are best addressed in the context of prospective multivariate modeling that takes into account potential demographic confounds and allows for dynamic meditational chains.
Endnotes
- The estimated total effects for depression were also modest. The total effect for the contrast comparing pooled kin/non-kin adoptions to non-adopted youth during young adulthood was 0.04. The total effect for depression during early young adulthood was 0.03.
- The total effect for the contrast comparing later adoptees to non-adopted youth on depression was 0.23 during early young adulthood and 0.12 during young adulthood. The corresponding effects comparing early adoptees to youth who were not adopted during early young adulthood was 0.04 and 0.03, respectively.
Authors Note
Trudy Festinger is a professor in the Silver School of Social Work, New York University.
James Jaccard is a professor in the Silver School of Social Work, New York University: jjaccard@gmail.com
Correspondence regarding this article should be directed to Dr. Trudy Festinger, New York University, Silver School of Social Work, 1 Washington Square North, New York, NY 10003-6654 or via e-mail to trudy.festinger@nyu.edu
Acknowledgement
This research used data from the Add Health study that was funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23
other federal agencies and foundations. No direct support was received from grant P01-HD31921 for this analysis.
PDF and Refrences: Suicidal Thoughts in Adopted Versus Non-Adopted Youth: A Longitudinal Analysis in Adolescence, Early Young Adulthood, and Young Adulthood